身為臨床的物理治療師
我們一直被被教導中立位置的重要性
從脊椎中立一直到關節的中心化
幾乎所有的評估治療運動
都是遵循這個原則
As a clinical physical therapist,
I was always taught that the importance of the neutral position.
From neutral spine to joint centration,
almost all evaluations, treatments, and exercises are follow this rule.

但有些時候我們在臨床上也會發現
即便個案能夠維持中立位置
他的疼痛依舊存在 或者沒有辦法根除
特別對於新畢業的治療師來說
這是一個相當大的關卡
But sometime we might found that
even the client can maintain neutral position, the pain is still existed.
It's a huge WHY, especially for new grad therapists.
為什麼病人對稱中立 但還是會感到疼痛呢?
Why the patient is still hurting after I did everything to make them neutral?

如果可以 我很希望在更早的時候就能了解這個重要觀念
"中立位置只是治療的起點"
I wish I could know this important concept earlier
"Neutral is just the starting point"
打個比方來說
你要去的方向是台北 但卻意外的到了高雄
這時單純回到原點無法解決問題
而是要從你的起點重新出發
Let's make it more solid.
If you want to get to NYC, but somehow you go to the Boston,
then back to where you began can not make you to the goal.
You have to START FROM THE ORIGIN

同樣的道理
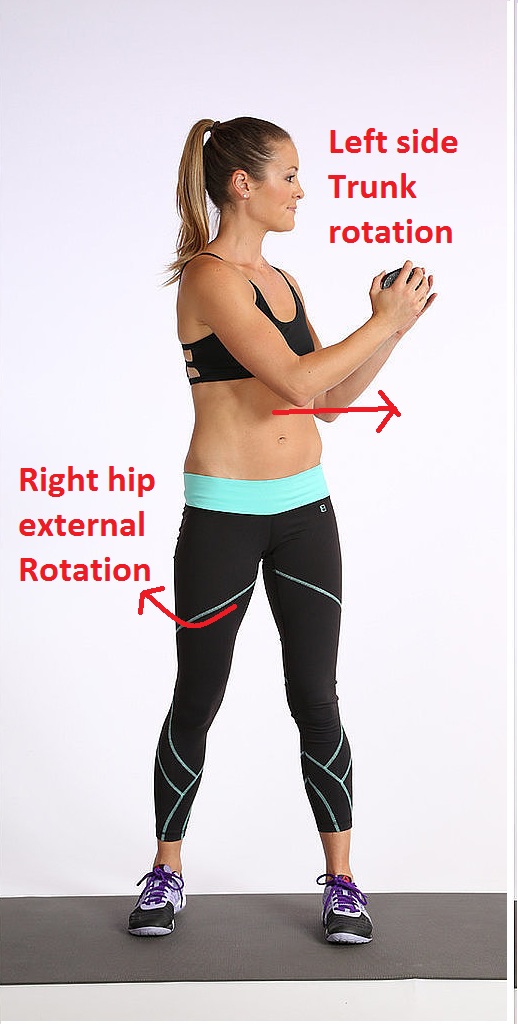
今天如果遇到了一個下背痛屈曲耐受不足的個案
你不單單要把他帶回脊椎中立的位置
同時需要讓脊椎能夠重新正確的體驗伸展/屈曲的動作
單純的中立而缺乏正確的訓練只會讓身體重新反覆錯誤的使用模式
So in the clinic,
if you meet a client who is suffer from LBP with flexion intolerance,
you can't just bring them back to the neutral spine.
They need to experience the real flexion/extension movement.
Simply put them back the the neutral without proper training can only lead to the repetitive problem.
Dr. Dooley在講課時說過
“到達他們所在的位置, 然後帶領他們到需要的地方”
我們要抵達的地方不該只是半路的中立位置
而是在更遠那一端的動作
Dr. Dooley has some amazing words
"Meet them where they are, bring them where they are not"
We shouldn't stop at the neutral,
we should guide them to where they truly should be.

本著作由I-Chen Liu, PT, MS製作,以創用CC 姓名標示-非商業性-相同方式分享 4.0 國際 授權條款釋出。